Contents
Introduction
Specimen Preparation
Description
Block Taking
Introduction
Although some elements of the description and cut up of a colorectal excisions specimen are specific to the type of specimen, there are some aspects of the preparation and description that are common to all types of specimen.
Preparation of the Specimen
The specimen needs to be allowed to fix properly. This typically requires at least 24 to 48 hours in a sufficient volume of formalin. Many of the key features of colorectal pathology are located in the mucosa and therefore access of the formalin to the mucosa is crucial. This is achieved by opening the specimen soon after receipt.
The specimen will often contain faecal material. This must be removed and washed away in order to prevent the faeces from acting as a barrier to the penetration of the formalin. Caution should be exercised when washing the specimen in order to avoid traumatising or avulsing any polypoid lesions.
If no tumour is present, the specimen can be opened by cutting along the bowel, opposite the mesentery (antimesenteric border) for the entire length of the specimen. This exposes the entire mucosa to formalin.
If a tumour is present, the opening should begin proximally and extend to just before the tumour. The tumour itself is not opened. In the case of an anterior resection the bowel distal to the tumour is often left closed as well; for resections from other parts of the large bowel, the distal aspect may also be opened close to, but not into, the tumour. A rolled up piece of absorbent paper can be inserted as wick through the lumen inside the tumour to facilitate penetration of formalin into the tumour.
The prevailing dogma is that the tumour should be left closed in order to preserve the integrity of the serosal surface and any circumferential margin.
If any perforations are present, the cut made to open the specimen should not pass through the perforations.
Inking of margins is discussed in the section on block taking.
Fixation of the specimen may be facilitated by pinning the specimen in an opened state to a cork board.

|

|
|
Fresh large bowel resection.
|
Large bowel resection after fixation.
|
Description
It should be noted that although the macroscopic description is often not dictated until after the specimen has been opened, it is necessary to commence the process of observation in order to determine how the specimen should be opened.
The basic macroscopic description should state the type of specimen. This may simply be a 'segment of large bowel', but for a right hemicolectomy it should be possible to identify the specimen specifically due to its unique morphology.
The length of the bowel should be given. Either the circumference or diameter should be measured. The distance to which the mesentery extends beyond the bowel wall should be noted.
A comment should be made on the serosa, if only to indicate that it appears to be normal.
Right Hemicolectomy
A right hemicolectomy will feature the caecum and ascending colon and a portion of terminal ileum. The length and circumference / diameter of each of these components should be given. The presence or absence of the appendix should be stated; if the appendix is included, its length and diameter should be given.
If a 'bare area' is discerned, this should be mentioned.
Anterior Resection
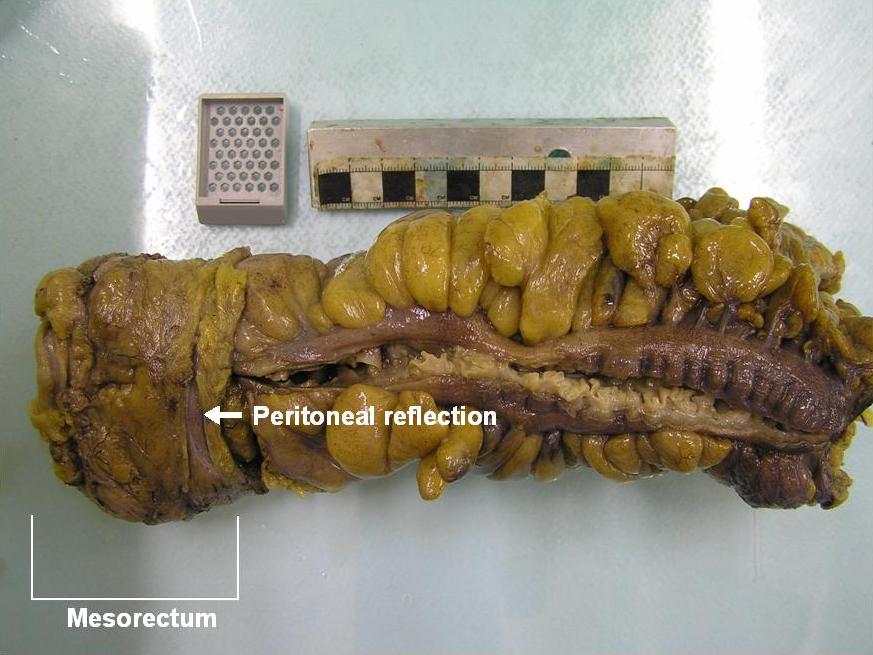
The rectum is located in the pelvis and much of it sits beneath the peritoneum. The peritoneum thus descends over the anterior surface of the lower sigmoid colon and upper rectum then curves (reflects) back upwards to cover the top of either the bladder in a male or the uterus in a female. This curve is known as the anterior peritoneal reflection. Beneath it the entire rectum is enclosed by the mesorectum and thus possesses a continuous circumferential margin.
|
|
An anterior resection.
|
Above the anterior peritoneal reflection the mesorectum comes to an apex on the posterior aspect of the rectum. As with the surface below the peritoneal reflection, the surface of this pyramid of mesentery is a surgical circumferential margin and is of prognostic significance.

|

|
|
Anterior resection viewed mainly from the front.
|
Posterior view of the circumferential margin of the same anterior resection.
|
The additional features of the description of an anterior resection relate to the mesorectum. The position of the anterior peritoneal reflection in relation to the proximal and distal margins should be stated. It is also required to comment on the nature of the mesorectal margin. The desired aim at surgery is to excise the entire mesorectum. This should yield a relatively smooth, uniform mesorectum. This can be described as 'the mesorectal plane of excision', although a form of words along the lines of 'the mesorectal surface is regular, implying the mesorectal plane of excision' perhaps acknowledges the realities better. In some instances, the mesorectal margin may be irregular, requiring the description 'intramesorectal' and rarely the mesorectal margin may cut into the muscular wall of the rectum itself ('intramuscular'). Assessment of the state of this margin is considered to be an important aspect of the quality control of colorectal surgery.
The CRM should be inked, preferably using one colour for the right side and one for the left. In order to assist orientation of megablock sections, a thin strip of a third colour may be used to mark the posterior midline.

|
|
|
An inked mesorectal margin.
|
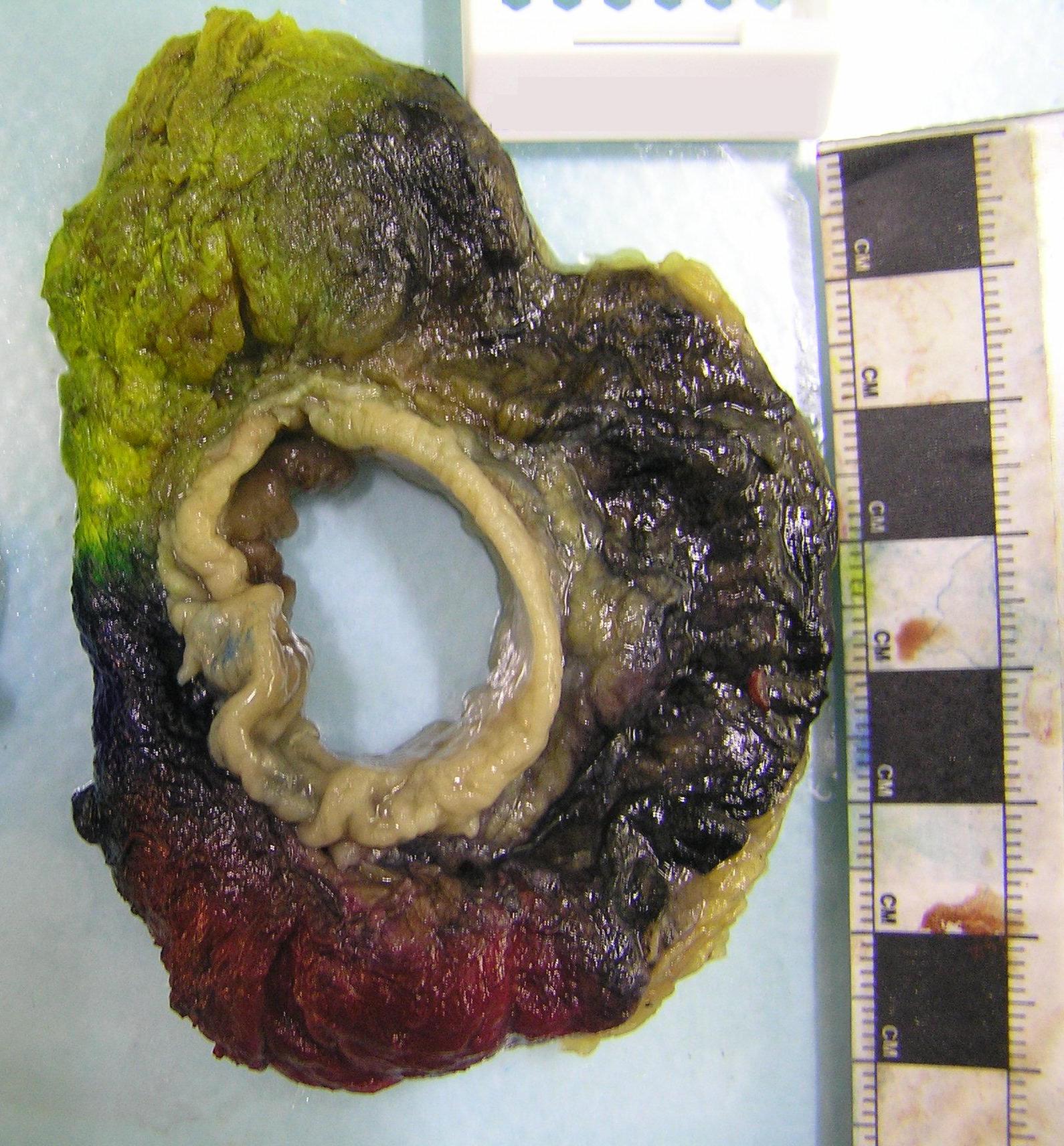
Differentially inked transverse section.
|
Block Taking
Colorectal resections fall into the category of
hollow organs and the basic principles of block taking for those organs apply.