Anatomy
The breast is also known as the mammary gland and is traditionally described as a modified sweat gland that has developed in order to allow mammals to lactate and suckle their young. It is fully developed only in postpubertal females.
The breast is located on the anterior chest wall and spans the region from the second to sixth ribs and between the lateral border of the sternum and the mid axillary line. The majority of the breast overlies the pectoralis major muscle from which it is separated by a layer of fascia; a small portion of the breast overlies the serratus anterior and external oblique muscles.
The axillary tail is a portion of breast tissue which extends up towards the axilla.
The nipple is located relatively centrally on the skin of the breast and is the structure through which milk is expressed. It is surrounded by the areola, which is an approximately circular region of skin that is more pigmented than the rest of the skin. The pigmentation is due to eumelanin (brown) and pheomelanin (red) and becomes particularly developed once menstruation commences. It can also be enhanced by pregnancy. The areola also features numerous sebaceous glands which are not associated with hair follicles. These sebaceous glands help to lubricate the nipple. They are sometimes referred to as Montgomery's tubercules.
Smooth muscle is present within the nipple and has an erectile function.
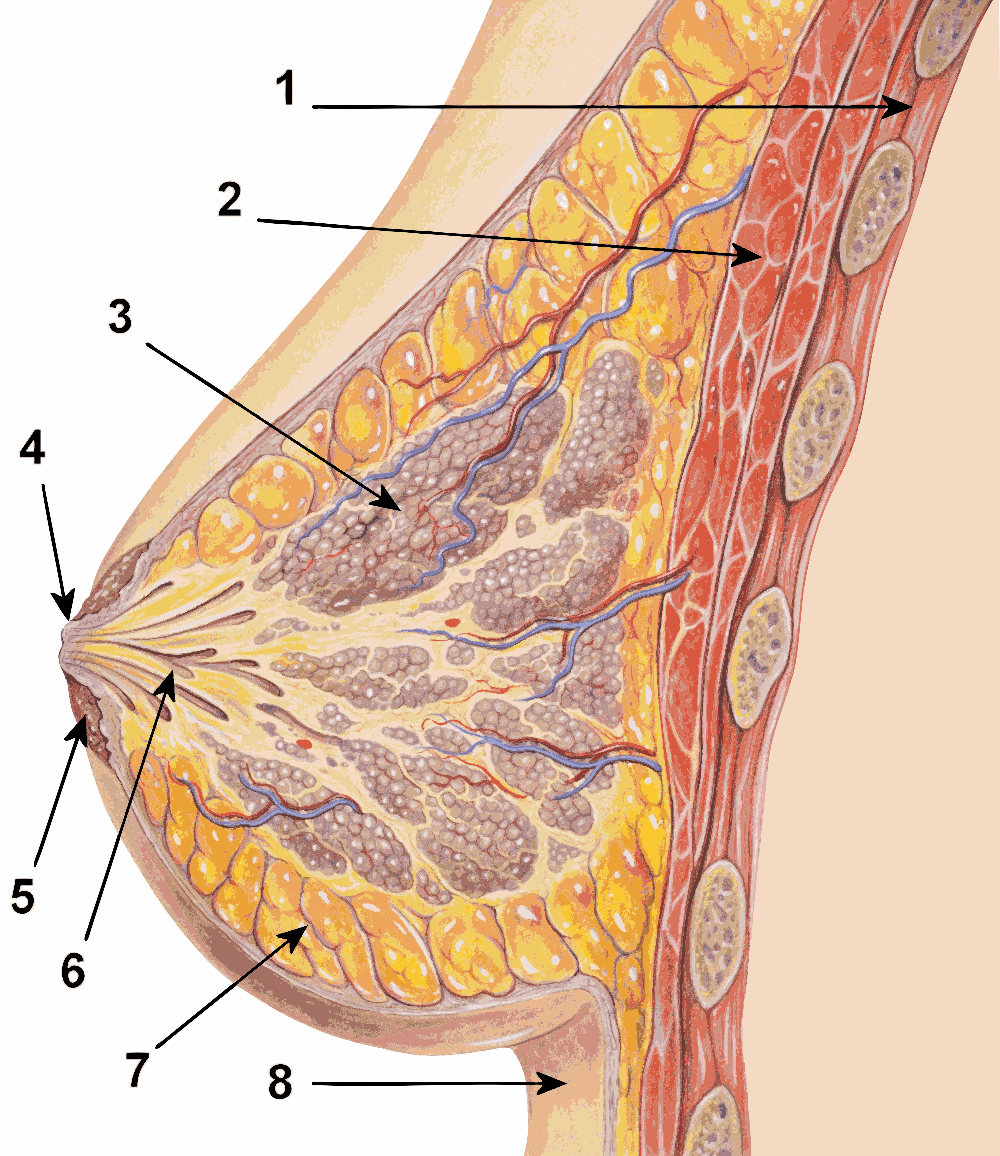
The basic structural anatomy of the breast is based upon a lobular architecture, although this is not readily apparent macroscopically. Each lobule is composed of multiple acini which drain via ductules into ducts that ultimately feed into the lactiferous duct which open through the nipple. The number of lobules and lactiferous ducts is around 10-20.
The terminal duct-lobular unit is the distal part of the breast lobule and is where the glandular acini that synthesise milk are located. The ducts and acini of the breast have a bilayered epithelium. The outer layer is formed by cuboidal myoepithelial cells that possess contractile properties. The inner layer tends to be cuboidal within the acini and becomes colunar within the ducts. The inner layer of cells in the acini is responsible for manufacturing milk. The epithelial component of the breast is supported by a connective tissue stroma. The epithelium possesses a basement membrane.
The tissue between the lobules is predominantly mature adipose tissue.
|
1 - Chest wall
2 - Pectoralis major
3 - Breast lobule
4 - Nipple
5 - Areola
6 - Lactiferous duct
7 - Mature adipose tissue
8 - Skin
|
|
Diagram courtesy of Wikipedia
|
The upper part of the breast features thickened regions of the fibrous connective tissue. These thickenings run from the breast to the fascia overlying the clavicle and the upper part of pectoralis major. They are known as the suspensory ligaments of Cooper and have a role in supporting the breast.
The blood supply of the breast is provided by the internal thoracic artery (internal mammary artery), the intercostal arteries and branches of the axillary artery. The internal thoracic artery is an early branch of the subclavian artery that runs downwards behind the ribs just to the side of the sternum.
The lymphatic drainage is mainly to the axillary lymph nodes, although a minority of the drainage is to the internal thoracic lymph nodes which are associated with the internal thoracic artery.
The breast is innervated by the second to sixth intercostal nerves. The nipple is in the T4 dermatome. The skin of the breast, especially the nipple, has a rich sensory innervation. The breast lobules are the province of the autonomic nervous system.
|
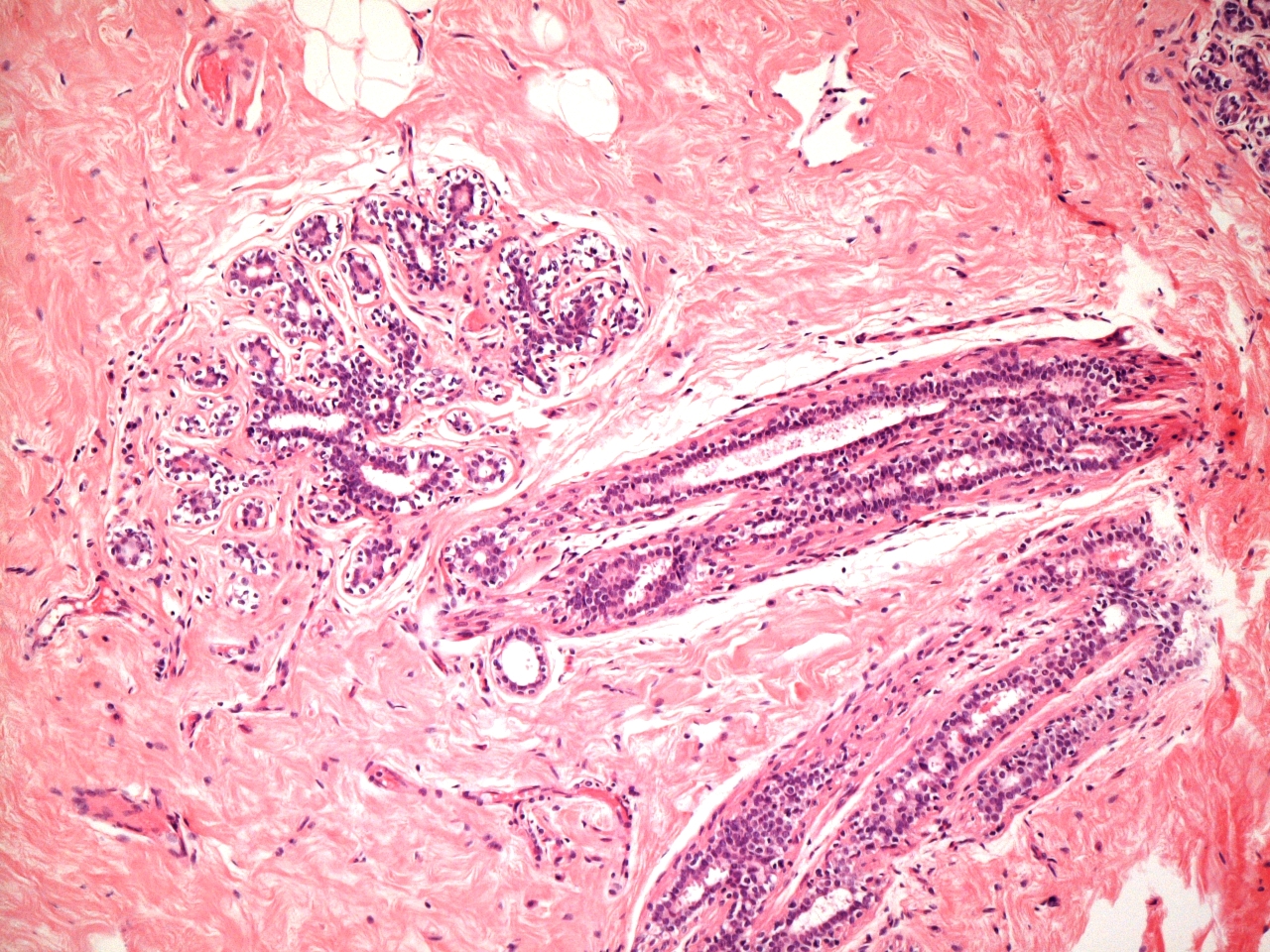
Microscopic image of a breast terminal duct lobular unit.
The myoepithelial cells are accenutated by clearing of their cytoplasm.
|
|
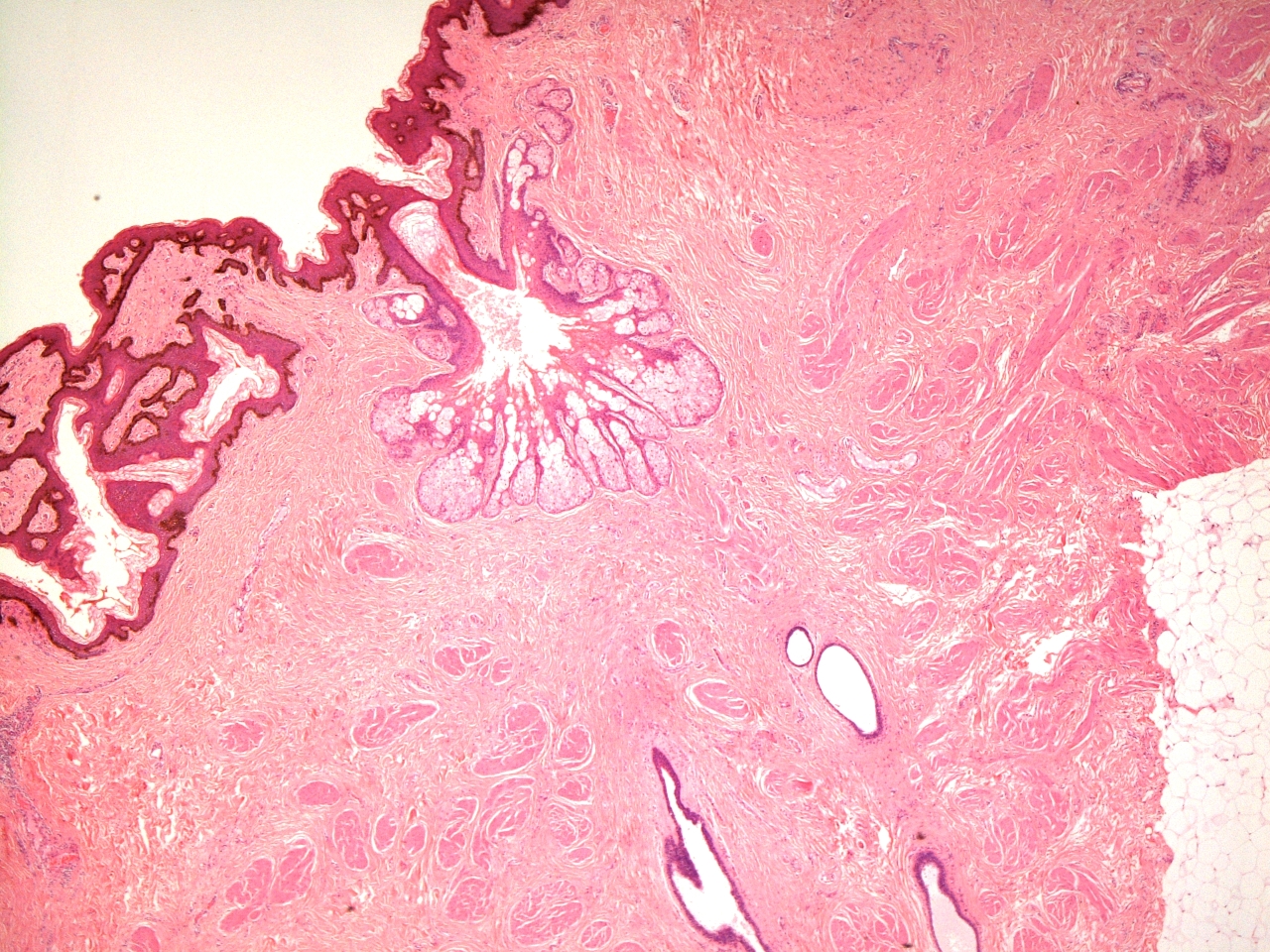
Microscopic image of the areola.
|
Development
The onset of the maturation of the breast during puberty is known as thelarche and usually occurs around 10-11 years. It is stimulated primarily be oestrogen; growth hormone and prolactin provide support.
The development of the breast is achieved by the expansion of the ductules to generate terminal duct-lobular units; the breasts of males and prepubertal females contain ducts without lobular units. The quantity of connective tissue and mature adipose tissue is increased.
The mature breast is generated from a disc of subareolar tissue. Excision of this tissue prior to the onset of thelarche will prevent the development of the breast.
From an embryological perspective the breast is derived from a structure known as the milk line (mammary ridge). This is a thicknening of the epidermis that runs from the axilla to the groin on the anterior surface of the body. One milk line is present on each side of the body. The nipple develops on the milk line. In humans, only one nipple develops on each side. For mammals as a whole the number of nipples is approximately twice the number of offspring on average produced by each pregnancy. Supernumerary nipples can develop anywhere along the milk line and may be associated with underlying breast tissue.
Physiology
The physiology of the breast is the process of lactation. In its resting state, the breast does not normally lactate and only undergoes modification into the lactating condition during pregnancy.
Various hormones control the conversion of the breast to a lactating state.
Prolactin causes hyperplasia of the breasts and stimulates the synthesis of milk. Oestrogen stimulates growth of the duct system and progesterone stimulates hyperplasia of the glands. The high levels of progesterone which occur during pregnancy also inhibit the actual synthesis of milk by the breast when it would be an unnecessary expenditure of resources but when progesterone levels drop after delivery this brake is removed. Human placental lactogen also stimulates the hyperplasia of the breasts during pregnancy.
The actual release of milk during breast feeding requires the posterior pituitary hormone
oxytocin. Oxytocin is released in response to the sensory stimulation of suckling but can also be secreted in response to the sound of the baby crying. Oxytocin stimulates the contraction of the smooth muscle of the breast ducts, causing them to expel the milk. This is known as the let down reflex.
Prolactin and oxytocin work as a team. Prolactin instructs the breast to make milk and oxytocin stimulates the breast to release it. A few days into pregnancy local control mechanisms also operate in an autocrine fashion in the breast such that the expession of milk stimulates the production of more milk.
The initial form of milk synthesised by the breast is called colostrum; small quantities of colostrum may leak from the breast in the few days before delivery. Colostrum is more concentrated than normal milk and contains high levels of proteins (including immunoglobulins).
The table gives the composition of human breast milk.
| Fat |
| total (g/100 ml) |
4.2 |
| fatty acids - length 8C (% ) |
trace |
| polyunsaturated fatty acids (%) |
14 |
| Protein (g/100 ml) |
| total |
1.1 |
| casein 0.4 |
0.3 |
| a-lactalbumin |
0.3 |
| lactoferrin |
0.2 |
| IgA |
0.1 |
| IgG |
0.001 |
| lysozyme |
0.05 |
| serum albumin |
0.05 |
| ß-lactoglobulin |
- |
| Carbohydrate (g/100 ml) |
| lactose |
7 |
| oligosaccharides |
0.5 |
| Minerals (g/100 ml) |
| calcium |
0.03 |
| phosphorus |
0.014 |
| sodium |
0.015 |
| potassium |
0.055 |
| chlorine |
0.043 |
| Data courtesy of Wikipedia
|
Some drugs can be excreted in breast milk and this must be borne in mind when prescribing for lactating women.
The epithelial cells of the lactating breast have a distinct appearance from the resting breast. They contain numerous secretory vacuoles and can develop nuclear changes which can be confused with dysplasia if a history of lactation is not communicated. The lactating breast also exhibits hyperplasia of its epithelial components and an increase in the epithelium : stroma ratio.
The breast also undergoes a mild degree of hyperplasia during the latter part (secretory phase) of the menstrual cycle.